For the first time in over two decades, a worrying decline in the number of deceased organ donors has led to a fall in life-saving kidney transplants across the United States. This alarming reversal occurred despite significant progress in other areas, including a rise in living donations and hospitals becoming more efficient at using available organs.
A System in Paralysis: Scrutiny and Fear
Historically, when overall transplant numbers have fallen, it has been due to simultaneous drops in both living and deceased donations, often linked to economic recessions or the Covid-19 pandemic. However, the situation in 2025 presented a new and contradictory challenge. While living kidney donations increased and medical teams successfully transplanted more organs they might once have discarded, these gains were completely offset by a sharp four percent decline in deceased donor kidneys.
This drop, equivalent to 663 fewer donations compared to 2024, dragged the total number of transplants down. The cause is not a lack of people on the donor register, but a profound systemic issue within the transplant process itself. A wave of new federal oversight and intense media scrutiny, focused on rare but horrific cases where errors were made, has created a climate of fear and excessive caution.

A new report by the non-profit Kidney Transplant Collaborative suggests this environment has led to potential donors and their families withdrawing from registries in record numbers. Simultaneously, organ procurement organisations (OPOs), terrified of becoming the next scandal, have become overly hesitant, turning away from donors they would previously have pursued.
The Inflection Point: A Case That Shook Trust
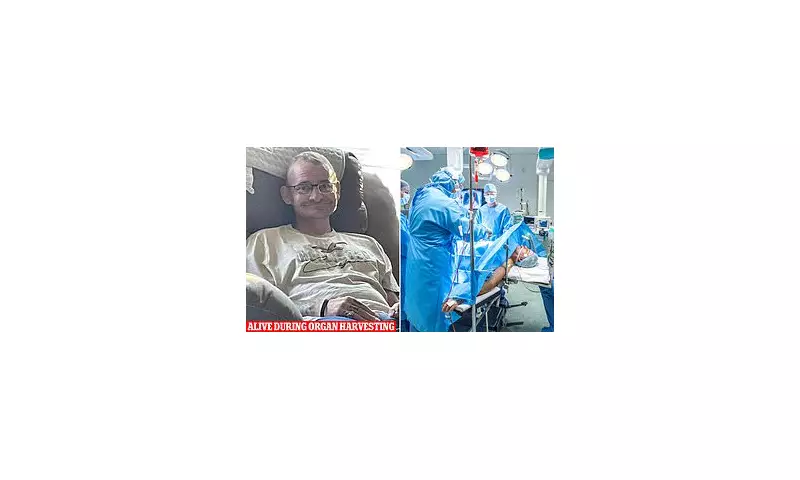
The report highlights a specific case, covered extensively by media outlets including the Daily Mail, that became a catalyst for this crisis. In October 2021, TJ Hoover was prepared for organ-removal surgery in a Kentucky hospital following a drug overdose. He had been declared a candidate for 'donation after circulatory death' (DCD).
Federal investigations and interviews with his sister, Donna Rhorer, revealed that Hoover displayed clear signs of consciousness – including tracking movement with his eyes and crying – as staff from the organ procurement agency allegedly pressed forward. The procedure was only halted when a hospital doctor refused to proceed, calling it inhumane. The incident left Hoover with permanent, profound cognitive disabilities.
This tragedy triggered comprehensive federal investigations by the Health Resources and Services Administration (HRSA) and congressional hearings. While the scrutiny aimed to correct grave safety failures, it has had a paradoxical effect. The intense focus on cases like Hoover’s has severely shaken public trust and made OPOs deeply reluctant to pursue DCD donors, where the determination of death is less absolute than with brain death.
This hesitation is critically damaging. DCD donations grew from 7% of deceased donor transplants in 2005 to 45% in 2024. By shying away from these donors and waiting only for brain death – which can take much longer or not occur – many potentially life-saving kidneys degrade and become unusable, directly shrinking the donor pool.
Consequences and a Proposed Lifeline
The decline, which began in June 2025, creates an immediate crisis for the roughly 94,000 Americans on the national kidney waiting list. The impact would have been even worse without a seven percent fall in the kidney discard rate, meaning hospitals used marginal organs more effectively.
Dr Andy Howard, Chair of the Kidney Transplant Collaborative, warned: ‘This is a serious signal for the transplant community and patients will feel the consequences quickly. The question now is whether we act in time to prevent avoidable loss of life.’

The report argues the solution is to pivot aggressively towards building a federally supported infrastructure for living donation. Its central proposal is to create a national system of ‘transplant facilitators’. These trained professionals would help candidates identify potential living donors and guide willing donors through every step, from screening to post-operative care, reducing drop-out rates.
Pilot programmes at institutions like Johns Hopkins and the University of Alabama show such support can make potential donors up to nine times more likely to complete screening. To implement this nationwide, the report calls for a crucial policy change: making facilitator expenses a reimbursable Medicare cost, just as Medicare funds deceased organ recovery.
Howard stated: ‘We know people want to be living donors. They're willing to do it, but we have to find a way to help them, and we feel the federal government needs to take action.’ With an ageing population increasing demand, the time to build this new lifeline is now.